
Dear Readers,
Below are the most commons in cardiology that I’ve put together from this block. I’m sure once I enter rotations I will be adding many more. Can I just say that one of my biggest pet-peeves right now is the incorrect pronunciation of medical terms? For example, angina. This word has been produced in two ways by various professors, but there must be a correct way to pronounce it, so naturally, I looked it up. “An-jen-uh” is the correct pronunciation, while “an-jine-ah” is colloquially used, but incorrect.
Cardiology Most Commons
- Most common pathologic process of the pericardium - Pericarditis
- Most common etiology of Acute Pericarditis - coxsackievirus A and B
- Most common cause of death in the U.S. - Coronary Artery Disease (CAD)
- Coronary microcirculation disease more common in women - this is why CAD affects more women than men annually
- Exercise electrocardiography less accurate in women
- More women die each year of CAD
- Most common cause of sudden cardiac death: ventricular fibrillation
- Most common cause of sudden cardiac death in young athletes: hypertrophic obstructive cardiomyopathy (HOCM)
- Hypertension
- More common in women as age increases
- More common in men in young and middle aged people
- More common in African Americans and lower socioeconomic groups
- African Americans develop at earlier age compared to other races
- Secondary HTN - more common in children
- White coat HTN - affects more treated women than men
- Obesity most common in African Americans, Hispanics, and Native Americans than Caucasians in US
- Resistant HTN - most common reason for referral to hypertension specialist
- Persistent BP 140/90+ despite treatment with full doses of 3+ classes of meds
- The most common cause of CAD is HTN
- The most common cause of right ventricular heart failure is left ventricular heart failure!
- Most common reason patients 65+ are hospitalized each year: congestive heart failure (CHF)
- Most common etiology of LV systolic dysfunction: CAD
- Most common secondary cause of dyslipidemia: diabetes/insulin resistance
- Most common etiology of mitral stenosis: rheumatic heart disease
- Most common etiology of endocarditis: staph aureus
- More common in males living in urban areas
- Native valve infective endocarditis (IVDU) most commonly
- Affects the tricuspid valve +/- mitral or aortic
- Affects normal valves
- Most common microbe: staph aureus
- Native valve infective endocarditis (non-IVDU) most commonly
- Affects the mitral and aortic valves
- Abnormal valves affected (RF and bicuspid aortic valve)
- Most common microbe: strep mutans
Other Most Commons and Tips for Memorization!
- While automaticity is greatest at the SA node, conductivity is greatest in the Purkinje Fibers (4000 mm/s) and slowest in the AV node (200 mm/s)
- Pericardial Friction Rub - hallmark finding of acute pericarditis
- “Water bottle” configuration - CXR finding of pericardial effusion
- Clinical Presentation of Constrictive Pericarditis
- WADE (heart failure symptoms)
- Weakness
- Ascites
- Dyspnea
- Edema
- Increased JVP (without decrease upon inspiration)
- +/- Pericardial “knock” - early diastole, L sternal border
- Beck’s Triad - classic presentation of Cardiac Tamponade
- Decreased arterial pressure
- Distended neck veins
- Faint heart sounds
- Pulsus Paradoxus - decrease in pulse and systolic pressure (10 mmHg+) with inspiration; seen in cardiac tamponade, but also seen in hypovolemic shock, COPD, and pulmonary embolism; thus, it is non-specific and not good to rule in or out
- Order of Heart Sounds
- SEM-SOSS “some-sauce”
- S1, Ejection click, Midsystolic click, S2, Opening snap, S3, S4
- Mid-systolic (HAPI) Murmurs
- Hypertrophic cardiomyopathy
- Holosystolic (MTV) Murmurs
- “Carvallo’s Sign” - increase in murmur with inspiration
- Diastolic (ARMS) Murmurs
- “Austin Flint Murmur” - a diastolic rumble heard with chronic aortic regurgitation
- Peripheral Pulses (Chronic Aortic Regurgitation)
- Waterhammer pulse (Corrigan’s pulse) - rapid increase in pulse
- Bobbing of head (de Musset’s sign) or uvula (Muller’s sign) with each heartbeat
- Quincke’s pulses (capillary pulsations)
- Traube’s Sign (“pistol shots” over femoral arteries)
- Duroziez’s sign (systolic and diastolic femoral murmurs)
- “Rule of 55” - operate before LVEF <55% or LV end-systolic dimension >5.5 cm
- For more advanced learning, the American College of Cardiology has Heart Songs for purchase available through their website. While it is expensive, you might consider purchasing this one as a group and sharing it amongst students.
- 2007 European Guidelines for treating HTN: “It is not important how treatment is started, but very important that BP goals are achieved”
- CHADs2 Score - Atrial Fibrillation Stroke Risk
- CHF = 1 Pt
- HTN = 1 Pt
- Age 74 + = 1 Pt
- DM = 1 Pt
- Secondary Embolic (stroke) Event: 2 Pts
- Cardiac Tamponade
- +/- in Pericardial effusion
- Medical Emergencies in Cardiology
- Cardiac Tamponade
- Ventricular Tachycardia - sudden cardiac death
- Ventricular Fibrillation - sudden cardiac death
- Hypertrophic Obstructive Cardiomyopathy (HOCM)
- Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
- Wolff-Parkinson-White Syndrome
- QT Prolongation
- Severely elevated BP (HTN) + acute or rapid organ dysfunction
- Various EKG Findings (keep in mind this is from a very basic understanding)
- Atrial Flutter - “sawtooth pattern” or “rapid regular”
- Atrial Fibrillation - “wavy baseline” “rapid irregular” “CHF promotes A-fib, A-fib aggravates CHF”
- PVC - “wide, bizarre QRS complex”; inverted wide-QRS; inverted T-wave; no p-wave;
- Wolff-Parkinson-White Syndrome - delta wave
- Idioventricular rhythm - “slow v-tach”
- Chronic Unstable Angina - 1 mm horizontal or down sloping ST segment depression in V5
- NSTEMI - ST segment depression + T-wave inversion
- STEMI - ST elevation
- Acute Myocardial Infarction
- Active injury: ST elevation, wide/deep Q wave, R wave normal, T-wave peaked
- As heart necroses: deeper Q-waves
- Post-injury: ST very elevated, R wave notching and loss of amplitude
- T-wave inversion within hours and before ST segment isoelectric
- ST elevation returns to normal within hours
- Depressed PR segment
- Acute Pericarditis - ST elevation/T-wave inversion (lasts days), decreased QRS amplitude
- Pericardial Effusion: decreased QRS voltage, QRS alterans
- Chronic Pericarditis - decreased QRS voltage, T-wave inversion
- Cardiac Tamponade - decreased QRS voltage
- Left Ventricular Hypertrophy (LVH) - thick lines, increased QRS voltage
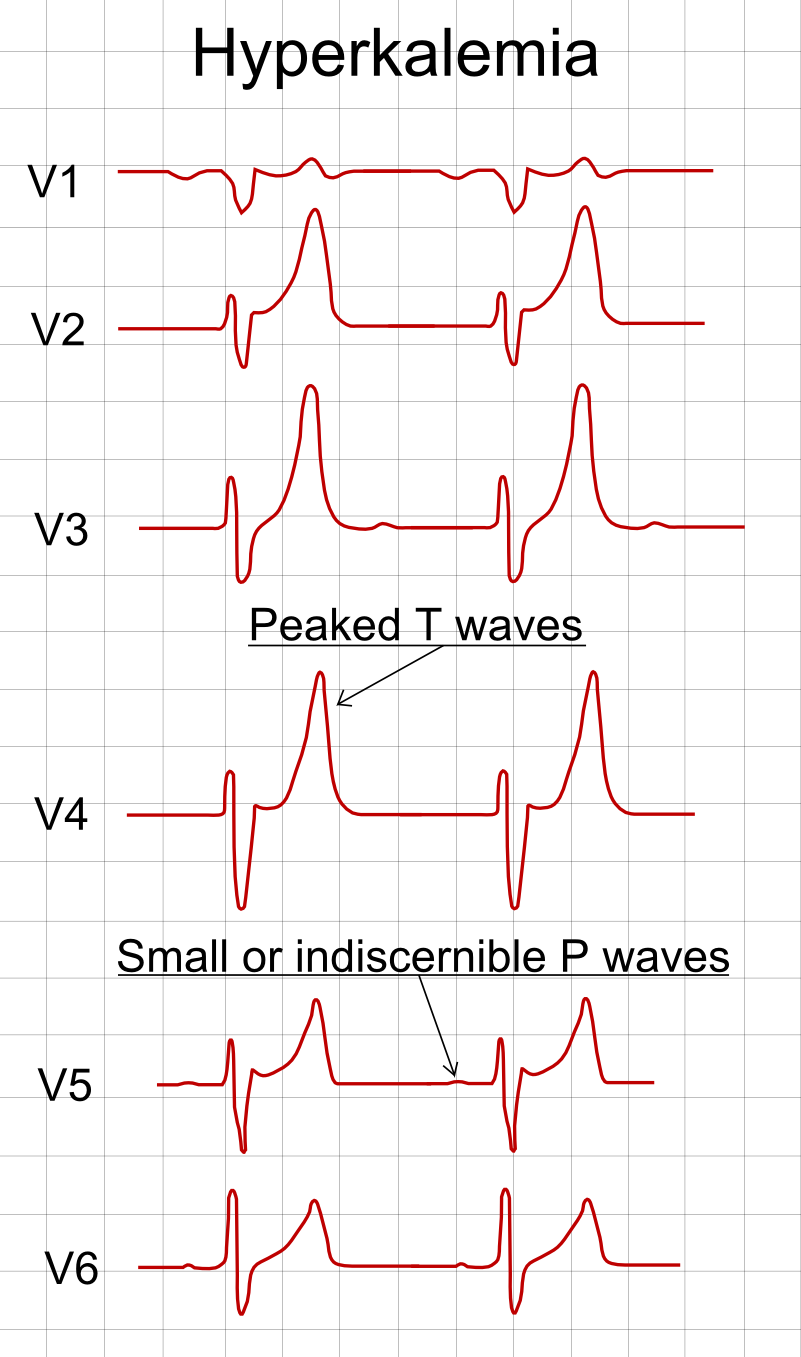
- Hyperkalemia - tall T-wave, sine-wave
- ST depressions + deep T-wave inversions - HCM (apical variant)
- ARVD (arrhythmogenic right ventricular dysplasia) - Epsilon waves
- Takotsubo “octopus trap” Cardiomyopathy is sometimes referred to as the “broken heart syndrome” or “stress cardiomyopathy” - mimics MI without CAD present
- Obviously patient history and physical exam are going to be more important in these cases, but here is a comparison that can be useful for remembering labs. This will especially be helpful in your ED rotation.
- Remember for sensitivity and specificity:
- SNOUT (SeNsitivity - rules OUT)
- SPIN (SPecificity - rules IN)
{kind=link}
Diagnosis | Identification/ Detection | Extras |
Acute Pericarditis | TTE | |
Chronic Constrictive Pericarditis | R-heart Catheterization | |
CHF | BNP (rule IN) | Increases with sepsis, pulmonary emboli Decreases with obesity |
AMI | Myoglobin (rule OUT) CK-MB (rule OUT) Troponin (rule IN) | If all 3 elevated - acute phase of MI |
NSTEMI | CK; CK-MB Troponin |
Sources:
0 Response to "Cardiology List of Most Commons for Physician Assistant Students"
Post a Comment