
Fifth Semester at UTSW
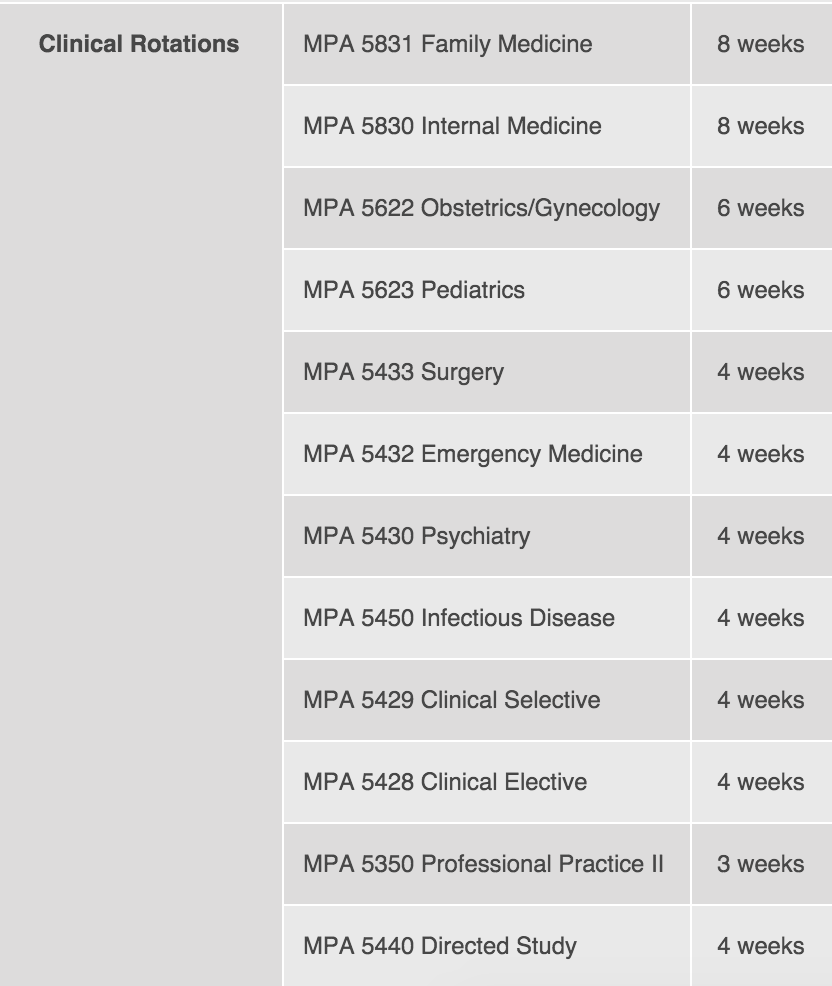
Below is a schedule taken from our program website detailing the clinical rotation schedule. Each student’s rotations are already set up for them (a huge plus), as I learned at the PAEA conference this year that not all PA programs do this. Some programs require that you setup your own rotations. Additionally, I appreciated an increased level of security that our rotations were quality - something not all programs ensure. Our rotations have been vetted before, dropping sites and preceptors who do not meet a high enough standard for our students. Our clinical coordinators have also done a great job of ensuring preceptors provide feedback to our students and that we get the most experience on each rotation, never being left in the shadows.
This year our class also joined the many PA programs utilizing PAEAs end-of-rotation (EOR) examinations, streamlining the examination process and unifying rotation evaluation with an enhanced & secure online experience mirroring the PANCE. After each 120-question exam we received feedback about our performance, including a topic list of each type of question we missed and the task area. The content of the exams is provided by PAEA in a blueprint style and topic list format.
MPA 5623 Pediatrics
Coming into my pediatrics rotation, I was very apprehensive. I’ve never considered myself to be playful enough and I could never tolerate the crying and screaming since I worked at a summer camp 8 years ago. My clinic changed those feelings for me and helped me realize that pediatrics isn’t as bad as I thought it would be. Getting to see my own patients on the second day, taking histories & performing physical exams, and creating asthma plans was suddenly a lot more exciting. I realized that in pediatrics you don’t have to manage a lot of comorbid chronic conditions, like diabetes and hypertension, or at least not as often as in the adult population. On August 10th, 2015, I began my first clinical rotation in PA school at a local pediatric clinic. The clinic served predominately Hispanic and African American patients and was 95% spanish-speaking only, reaching an underserved area of Dallas, mostly including Medicaid and cash-only paying patients without insurance. My pediatrics rotation lasted 6 weeks and included a visit to the Dallas Children’s Advocacy Center (DCAC) where we learned about recognizing and reporting child abuse through lecture discussion, video, and a tour of the facility. The rotation also included a visit to the REACH clinic at Children’s Medical Center where we were able to gain a more in depth and sensitive coverage of child abuse. The rotation concluded with a presentation (review) with other students on various topics in pediatrics and included creation of 2 handouts and an oral presentation. Below is a review of the “core-task areas” we are expected to cover in each rotation and for each I listed what my objectives were & how I met those objectives.
PATIENT CARE
My goals for pediatrics were to review topics I was unfamiliar with, such as the pediatric milestones, immunization schedule, primitive reflexes and postural reactions. I practiced these with several children and went over them with the MAs on a routine basis to become more familiar. It was also my goal to be able to recognize and differentiate pediatric rashes from one another and to practice clinical skills that aren’t performed in a hospital setting. My preceptor did a great job explaining how rashes present and how the history may differ. Some of skills I performed included administering injections, performing rapid strep antigen testing, urine hCG testing, CBCs, urinalysis and more. My goal was to become familiar with the tests’ implementation, rather than just recognizing when to order them. I also wanted to develop my own management plans; asthma, for example, which I did. In this clinic, we didn’t perform many surgical procedures due to a lack of equipment. We did refer to other specialists where we couldn’t take action and learning my own limitations was a useful quality to adopt.
MEDICAL KNOWLEDGE
My own ability to identify signs and symptoms of medical conditions, such as skin rashes and viral illnesses based on history and physical alone improved significantly. One of my goals was to be able to interpret laboratory studies and formulate differentials based on given risk factors, etc. I now feel more comfortable diagnosing eczema, contact dermatitis, insect bites, tinea, hand-foot-and mouth, scarlatina and other viral exanthems. Dosing medications was entirely new since this was my first rotation, but I would ask my preceptor to help me dose simple medications, such as Amoxil, Keflex, Tylenol and Motrin, which we prescribed a lot.
PRACTICE-BASED LEARNING AND IMPROVEMENT
My goals for this rotation were to identify and implement evidence related to patients’ specific health problems, which I felt I was able accomplish. I actually created 4 pamphlets in Spanish for our patients on fungal infections, scabies, warts, and acne, which are all very common. I was also able to research and present orally to my preceptor on the etiology, presentation, pathophysiology, and treatment options for diabetes. We both benefited from learning more about diabetes, as we did not really manage it much in clinic. Overall, I was able to learn a lot more about my patient population (mainly Hispanic) and the larger population they are drawn from (low income). Unfortunately, I was not able to create a study design or apply statistical methods to improve therapeutic effectiveness. I had planned to do an in-service for our MAs and to help improve vitalization errors, but we had such a high turnover in MAs that it made it nearly impossible. I was able to learn how to document and bill for diagnoses and procedures, but only to an extent. I hope to learn more in the future.
INTERPERSONAL/COMMUNICATION SKILLS
Communication was a huge barrier for me at the beginning of my rotation, but I almost feel that I attained better communication skills than medicine in this rotation. I’m not sure if that is a good or bad thing, but I know that I took away a lot of medical Spanish and I feel 100% more comfortable seeing my own Spanish-only speaking patients with a few exceptions. I also learned a lot about how you must adapt your communication style to a 4 year-old versus a 15 year-old patient and how you must adapt your physical examination techniques using the otoscope and ophthalmoscope in younger children. This rotation helped me overcome fear of giving injections and holding infants, which previously made me very nervous since children are so fragile at young ages. I learned to remove my own biases and learned how to treat the patient, instead of their lingering on their illness.
SYSTEMS BASED PRACTICE
Unfortunately, some of my patients were cash patients, which made it extremely difficult to order tests and prescribe appropriate medications. I learned how to adapt care to provide improved quality of life for those children without insurance. I also learned a lot about Medicaid and the different plans, including Amerigroup, which stopped covering Singulair recently. Lots of our patients were on Singulair and were shocked to find out their child could no longer receive the medication, as it was too expensive for them to afford out of pocket. My preceptor and I were resilient, though, and we came up with other options for each patient’s asthma plan. Occasionally, we could get exception forms signed by Medicaid. I also learned about how diagnoses determine what labs and medications are covered, which sometimes must be altered in order to obtain appropriate therapeutic intervention. We practiced as cost-effectively as possible and I realized that our healthcare system still compromises quality of care because of limitations mentioned previously. I accepted these negative factors, but realized how diverse care is for private insurance patients, Medicaid, and cash patients.
MPA 5430 Psychiatry
Becoming acquainted to the jail-environment has probably been the most challenging and most influential part of my psychiatry rotation. While there, I learned how mental health is distributed across all races, sexual orientations, ages, and genders. Although certain groups may be predisposed to becoming incarcerated, the justice system is still faulty and the county jail really serves as a mental health institution where people can receive their treatment in a controlled environment without the distraction of external motivators. The jail has made me aware that no matter the circumstance or amount of education, people may live in the free world with mental disorders and function completely normal until a trigger “sets them off.” Mental health has a very negative stigma and connotation affiliated with it, leaving society less likely to maintain or manage symptoms until they are severe enough to warrant arrest. This is definitely one specialty that could use additional providers and a revamping process to make people feel less taboo or ostracized, and offer more of a supportive approach to management, including free resources for therapy, medication, and screening.
My psychiatry rotation lasted 4 weeks long and was at the local county jail. It wasn’t like you’d expect - it was safe, heavily guarded, and well-controlled. During the rotation we also attended weekly lectures given on psychotropic medications and law. The rotation also included a visit to an Alcoholics Anonymous meeting, which I will write about later, and we had the opportunity to observe electroconvulsive therapy on the inpatient side at Zale Lipshy University Hospital. Below is a list of the tasks required for the rotation and a little bit about the objectives for the rotation.
PATIENT CARE
My goals for psychiatry were to review DSM 5 topics and be able to make informed decisions about diagnostic and therapeutic interventions based on patient presentation, history, signs, symptoms, and clinical judgment. I was able to do this by developing interview and mental health history taking skills and discussing ongoing management of patient care with our preceptors.
MEDICAL KNOWLEDGE
My knowledge of the symptomatic presentation of the spectrum of psychiatric illnesses was limited upon entering psychiatry. I now have a broader sense of what is considered “malingering,” and how patients may manipulate your lack of clinical expertise by faking signs of illness. There are subtle changes to be noticed in psychiatry, including response to internal stimuli, which recognizing makes all the difference in the way we treat patients. I was also able to increase my knowledge of psychiatric differential diagnoses and compare the risk vs. benefits of adding, increasing, or removing psychotropic medications, many of which are based on side effect profile.
PRACTICE-BASED LEARNING AND IMPROVEMENT
I was able to incorporate information technology (IT) to manage health information by accessing online records (Epic and Pearl). With the aid of my preceptor, I was able to review literature of psychiatric topics, such as malingering, hallucinations in adolescents, and bipolar disorder in adolescents. I was also able to recognize when to use appropriate assessments, such as the BARS, MMSE, CIWA-Ar, COWS, Mini Cog and MOCA.
INTERPERSONAL/COMMUNICATION SKILLS
Throughout this psychiatry rotation, I was able to adapt my interviewing skills to each patient, recognizing that my own facial and emotional expressions play a large role in the interview. My anxiety initially peaked the first week as we adjusted to the jail-environment, but I shortly realized how safe and controlled the environment was with the extensive security protocols in place. The inmates were mostly very respectful and my experience in the jail has decreased my own bias toward the jail environment and delinquents overall. We learned about the legal system in our Law 101 class, which I greatly appreciated at the beginning of our rotation to aid my understanding of how inmates’ progress through the legal system, their medical appointments, their financials and the expanded terminology used.
SYSTEMS BASED PRACTICE
At the end of this rotation I realized the importance of mental health in the larger scope of a person’s overall well-being. I became aware of the societal barriers – lack of insurance, lack of access to treatment, lack of financial support, lack of family support, etc. that affect many of the inmates. Even within the county jail, there is a lack of mental health providers and liaisons – decreasing the treatment and therapies patients could be benefiting from while incarcerated. Even so, many patients return to the county jail because of lack of adherence to appropriate therapies and relapse into prior high-risk activities. The jail provides – at least to my knowledge – cost effective care. Many of the providers lectured us on how they prescribe medications based on what is cheapest to manage symptoms. Adjustments are made accordingly and treatment plans are patient-specific, as they should be. Overall, this was a very grounding rotation and I feel better prepared to approach mental health in my other rotations and my future.
MPA 5622 Obstetrics & Gynecology
Every time someone asks me, “how was/is your OB/GYN rotation?” I immediately think of something silly or pessimistic to say, because that’s what’s “expected”. I had a long talk about this after clinic one day with one of my residents, a male OB/GYN at my OB/GYN site, and we discussed how hard it is to be a male student or resident in women’s health because of this stigma. This was immediately following an incident where I performed a speculum exam in front of him and a female doctor with some difficulty.
Society suspects men interested in women’s health to either be 1) creepy or 2) weird, so it’s already a difficult learning environment for us. Half of our patients turn us away because they’d rather see a female and the other half are wondering what is going through our heads as we examine them because they can’t get over the fact that we look like someone they know. This resident gave me the advice not to let anyone, including a preceptor, deter my love for medicine or an interest in a field because of their own insecurities. I really appreciated that lesson because I felt very ostracized at many points – not just with that patient, but also from my preceptors. Language barriers presented a huge problem for my first 3 weeks of OB/GYN and I made it abundantly clear that I was not fluent enough to communicate at the level expected of me. It was really difficult to learn the language and the medicine at the same time. I did learn a lot of medical Spanish, but my preceptors did not allow me to practice as independently as I had wished because of my language deficit. I was able to use my medical Spanish during the OB portion of my rotation, which proved useful. Practicing really does make perfect, and I appreciate those preceptors that gave me the opportunity to practice with patients in Spanish, even if it wasn’t the best. Overall, this rotation has been a whirlwind of information and I have learned the most during this rotation than I have so far. It has been a great experience and I will always remember my first baby being delivered at 2:05 AM.
This rotation was another 6 week rotation and included weekly lectures on OB/GYN topics given by top specialists from each specialty from UT Southwestern. In addition, we also had a hands-on simulation lab the speculum exam. The first 3 weeks of my rotation were spent at an outpatient community health center in Fort Worth, where we had lectures on the ins-and-outs of community health centers. I primarily worked with a nurse practitioner who served as the sole gynecology specialist within the clinic, but I also had the opportunity to see outpatient OB patients. This community health center served a primarily Spanish-speaking only population who were also low-income and some undocumented citizens. The breadth of knowledge and experience I gained from this site is invaluable. The second 3 weeks was spent at Clements University Hospital on the Labor & Delivery unit for the OB portion of my rotation.
PATIENT CARE
Patient care goals for OB/GYN were to make clinical decisions and assessments of patients, perform gynecological procedures with the supervision and direction of preceptors, and become familiar with necessary clinical skills for the OB/GYN setting from prenatal assessment to post-partum care. I definitely felt comfortable performing gynecological procedures, but I am by no means proficient. For example, I could still improve the subtleties of my speculum exam, but I feel comfortable enough with completing well-woman exams, including bimanual and breast exams. I also had the pleasure learning to insert and remove IUDs and observing vasectomies and Implanon insertions. I was also able to take histories, perform physicals, and make clinical diagnoses on my own by the end of my rotation, which was my goal.
MEDICAL KNOWLEDGE
My knowledge of the symptomatic presentation of the spectrum of things like hypertension and diabetes in pregnancy was very limited prior to OB/GYN. MFM (maternal fetal medicine) and OB in general allowed me to really grow my medical acumen and understand the risk factors, pathogenesis, and clinical criteria behind the disease process in order to select the most appropriate diagnostics, treatment, or follow-up. I definitely became more proficient at developing a differential for common OB/GYN complaints.
PRACTICE-BASED LEARNING AND IMPROVEMENT
I was finally able to incorporate information technology (IT) to manage health information by accessing online records (Epic and NexGen), which I was previously very inefficient with. With the aid of many preceptors and residents, I was able to navigate the EMR with ease and learn how to properly document notes, bill, list diagnoses, order medications, send patient reports in MyChart, and much more. This is the first time I have ever felt comfortable using Epic and NexGen since starting clinical rotations and I attribute my success to many helpful and patient residents on my rotation. This is also the first time I have successfully completed a full H&P and documented my note electronically with full A&P, billing and coding added.
INTERPERSONAL/COMMUNICATION SKILLS
Probably one of the most important lessons of this rotation has been about interpersonal and communication skills. There have been some very emotionally challenging components of history taking on OB/GYN and other instances where I observed miscommunication between residents & nurses go awry. Ultimately, I have learned that a high stress environment can make almost anyone tense or edgy. We all have a choice in how we respond and demonstrating emotional resilience and stability can really have an impact as we set an example for our peers. I also learned that a little humility and a lot of altruism can go a long way, especially for someone who feels very unappreciated. These lessons were unanticipated, but very much appreciated and I feel like I have grown a lot from this rotation, realizing that clarity in speech is crucial and miscommunication always needs to be cleared up instantly.
SYSTEMS BASED PRACTICE
Working at a community health center definitely allowed me to become more familiar with outpatient settings for the undocumented, but also opened my eyes to another side of family medicine I never thought I’d enjoy. Serving a Spanish speaking underserved population has always been on my top list of “places to work” and this is one type of practice I never knew existed! I learned how CHCs are funded, how they operate, and whom they serve. This clinic was one of the most effective and well-run clinics I have ever been to in my life and I would expect half the level of care for any of my future patients that they provide. Not only do they advocate for an undocumented population, but the organization of the clinic itself and the well-trained MAs who work there are definitely something to brag about. I definitely look forward to working for a CHC in the future and I have this clinic to thank for introducing me to the setting.
0 Response to "Fifth Semester at UT Southwestern"
Post a Comment