
Introduction to Radiology for Physician Assistants
Updated: 06/09/2016
In this post, I hope to introduce you all to the differences between imaging modalities, including indications and contraindications. My goal is also to provide a basic understanding of the concepts surrounding density and normal x-ray findings. Future posts will investigate the findings for pneumonia, pneumothoraces, effusions, atelectasis, fractures/dislocations, arthritis, intracranial, GI and hepatic pathology, bowel, lines/tubes, and heart disease.
Conventional Radiography (Plain Films)
- Images produced through use of ionizing radiation
- No contrast material (barium or iodine)
- Why it’s important: Large doses of radiation can produce cell mutations leading to cancer or anomalies. Even low levels of radiation are teratogenic (avoid in pregnancy).
- Relatively inexpensive, obtained easily (portable, mobile), most widely used
- Common uses: chest x-ray (CXR), abdominal x-ray, and for fractures or arthritis
Computed Tomography (CT or CAT Scans)
- Uses a gantry with a rotating x-ray beam and multiple detectors with sophisticated algorithms to process the data
- Expensive equipment, lots of space, and high computer processing power required
Ultrasound (US)
- Uses acoustic energy above the frequency of human hearing to produce images
- Uses a transducer (produces and records signal), processed by a computer
- Inexpensive compared to CT/MRI, widely available, portable/handheld
- Very safe with no major side effects
- No use of ionizing radiation - great for women of childbearing age, pregnant women, and children
- Common uses: Used to image soft tissues and delineating solid from cystic structures, image-guided biopsies, non-invasive means to study blood flow
Magnetic Resonance Imaging (MRI)
- Utilizes potential energy stored in body’s hydrogen atoms (manipulated by magnetic fields and radiofrequency pulses) to produce localizing and tissue-specific energy
- 2 or 3-D images
- Not as widely available as CT, expensive, and high-operating costs
- No ionizing radiation, produce higher contrast between different types of soft tissue compared to CT
- Cannot use with objects within the body (pacemakers), ferromagnetic objects in MRI-scanner field (O2 tanks)
- Common uses: neurologic imaging, soft tissues (muscles, tendons, ligaments)
- Adverse effects from some MRI contrast agents
Terminology Conventions
- Most images are viewed as if you are viewing the patient face-to-face (no matter the position of the patient when the image was exposed)
- Ex. the patient’s R-side is on your L-side and vice-versa
- Study: collection of images to examine a particular part of the body or system
- Contrast material or agent: administered to a patient to make structures more visible
- Liquid barium (oral for upper GI exams and barium enemas)
- Iodine (IV for contrast-enhanced CT scans)
- Gadolinium (IV solution for MRI) and ultrasound (gas-filled microbubbles)
- Dye is a lay-term for contrast (only used if talking to a patient)
- Horizontal vs. Vertical X-rays
- Horizontal x-ray beams are parallel to the floor (duh!), also called upright chest examinations
- Why is this important? An air-fluid or fat-fluid level will only be visible if the x-ray beam is horizontal (regardless of the patient’s position)
- Any study with the terms: erect, upright, cross-table, or decubitus are by default horizontal
- Vertical x-ray beams are between the tube and cassette (supine radiographs)
Examples | Orientation | Implications |
Upright Abdomen | Horizontal | Air-fluid levels Free-air under the diaphragm |
Left lateral decubitus of Abdomen | Horizontal | Air-fluid levels Free-air over the liver |
Supine Abdomen | Vertical | Free-air only if large amounts NO AIR FLUID LEVELS |
Upright Chest | Horizontal | Pneumothorax at apex of lung Air-fluid levels |
Supine Chest | Vertical | Pneumothorax only if large NO AIR FLUID LEVELS |
The Five Basic Densities
- From least to most dense
Density | Appearance |
Air (black) | Absorbs the least (least dense) |
Fat | Gray, somewhat blacker than soft tissue |
Fluid or Soft Tissue | Both fluid (blood) and soft tissue (muscle) have the same densities on XR Note: cannot differentiate between blood/heart muscle on XR |
Calcium (White) | Most dense, naturally occurring material (bones) |
Metal (Whitest) | Absorbs all x-rays (bullets, barium), most dense |
White and Black
Terms for “White” | Terms for “Black” | |
Conventional Radiographs | Increased density or opaque | Decreased density or lucent |
CT | Increased (high attenuation) Hyperintense or hyperdense | Decreased (low attenuation) Hypodense |
MRI | Increased (high) signal intensity Bright | Decreased (low) signal intensity Dark |
Ultrasound | Increased echogenicity Sonodense | Decreased echogenicity Sonolucent |
Nuclear Medicine | Increased tracer uptake | Decreased tracer uptake |
Barium studies | Radiopaque | Nonopaque Radiolucent |
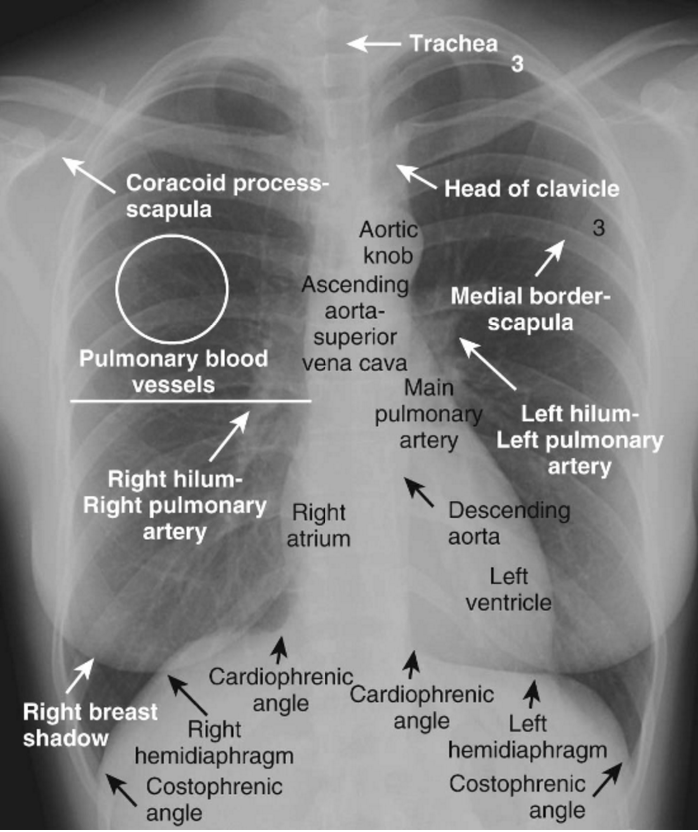
- Vasculature is seen as white lines on an x-ray (cannot differentiate pulmonary arteries and veins)
- Bronchi are invisible because they are thin-walled, contain air, and surrounded by air
- Pleura, composed of 2 layers and an inner pleural space, contains several mm of fluid but no air → neither are visible on XR (if they are, they are no thicker than a thin line)
2-Views (the Upright and Left Lateral XR)
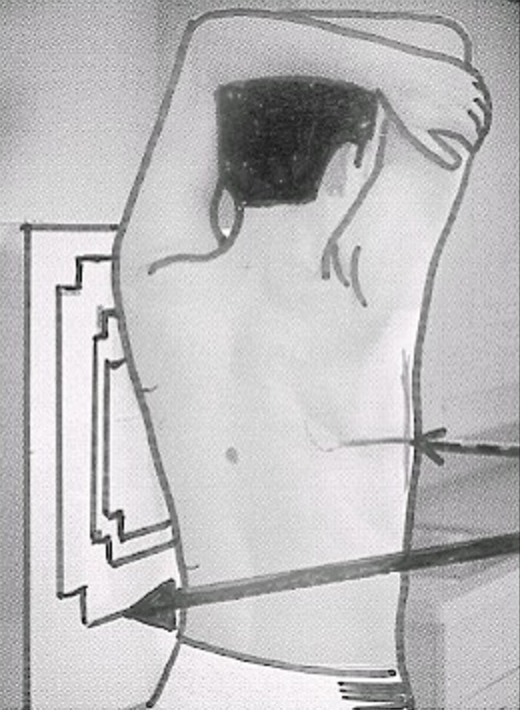
Left Lateral (left side against film): imagine you are looking at the patient’s right side, spine should be on your left
- Helps to determine location, confirm the presence, or rule out disease based on frontal (upright) XR findings
- Helps to visualize hilar densities (enlarged pulmonary arteries) or lymph nodes, which cast a distinct lobulated mass-like shadow
- Major (Oblique) and Minor (Horizontal) Fissures
- Both may be visible as fine, white lines and differentiate the upper and lower lobes on left, upper, middle, and lower lobes on right
- Major crosses obliquely through 5th thoracic vertebra to point on diaphragmatic surface of pleura a few cm behind sternum
- Minor fissure crosses at level of 4th anterior rib (R-side only) and is horizontal
- Only minor fissure seen on frontal view because of oblique plane of major fissure
- Degeneration can lead to narrowing of the disk space and development of small, bony spurs (osteophytes) at margins
- Right hemidiaphragm is visible in entire length (front-back) and is slightly higher than left
- Left hemidiaphragm is sharply posterior and is silhouetted by muscle of heart anteriorly
- Air in the stomach or splenic flexure of the colon appears immediately below the left hemidiaphragm
- Posterior costophrenic sulcus (angles) - each hemidiaphragm produces a rounded dome that indents the central portion of the base of the lung producing a sulcus (depression) surrounding the periphery of each lung
- Air in the stomach or splenic flexure appears below the left hemidiaphragm
- Note on frontal XR, these are called lateral costophrenic angles (sulci)
- Only requires 75 cc or less to blunt posterior angle on lateral films and 250-300 cc to blunt lateral angles on frontal
Five Key Areas on Lateral CXR
Region | Normal Findings | |
Retrosternal Clear Space | Lucent crescent between sternum and ascending aorta Note: do not mistake patient’s arms (superimposed soft tissue) for ‘filling in’ of clear space; occasionally patients are too weak to raise arms above their heads → if you see the humerus, it's an arm! | 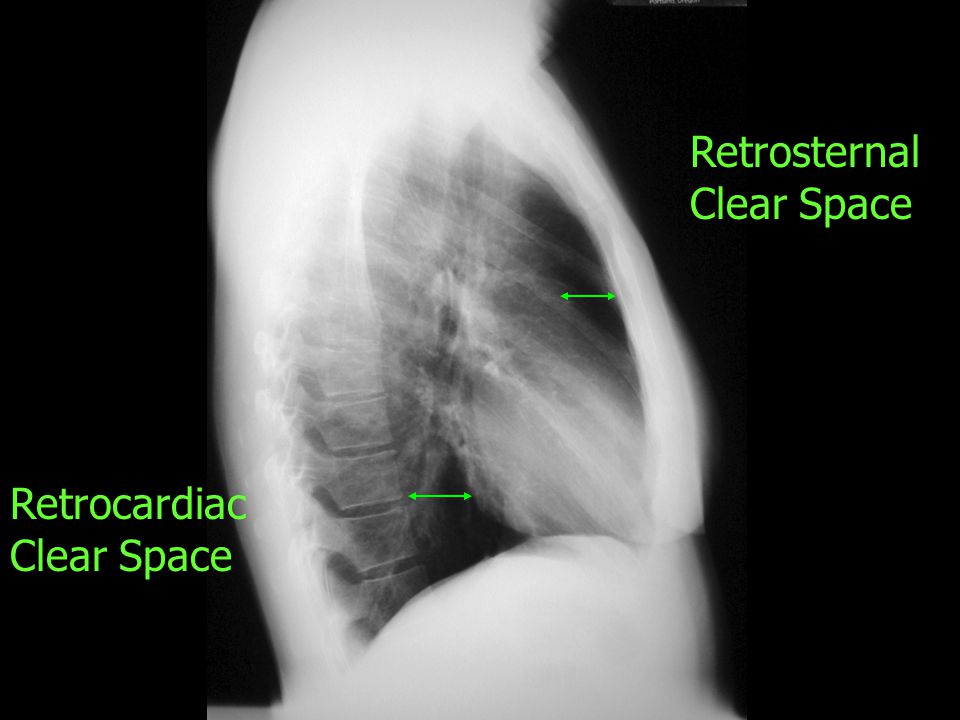 If obscured, think anterior mediastinal lymphadenopathy (most common) |
Hilar Region | No discrete mass present |  Look for a lobulated mass in region of the hila as shown above |
Fissures | Major and minor fissures should be pencil thin (if at all) |  Become thick with fluid (added Kerley B lines; think pleural effusions) or fibrosis (no other signs) |
Thoracic Spine | Rectangular vertebral bodies with parallel end plates Disk spaces maintain height from top to bottom, each becomes slightly taller than or remains the same height as the one above it |  Compression fracture = loss of body height |
Diaphragm and Posterior Costophrenic Sulci | R-hemidiaphragm slightly higher than left Sharp posterior costophrenic sulci |  Pleural effusions blunt the costophrenic angles |
The 5 Technical Factors - Is My X-ray Adequate?
- Underpenetration (inadequate): will appear too light and you won’t be able to see the spine through the heart shadow
- Left hemidiaphragm may not be visible on frontal XR, left lung base opaque, which can mask true pneumonia or pleural effusions → get a lateral XR to confirm
- Pulmonary markings may appear more prominent, leading you to think patient has CHF or pulmonary fibrosis → get lateral XR and look for increased markings, airspace disease, or effusion
- Overpenetration (too dark), lung markings appear decreased or absent
- Leads you to think patient has emphysema or pneumothorax → look for other radiographic findings to support your claim or repeat XR
- Degree of Inspiration - count number of posterior ribs above the diaphragm on frontal XR
- Posterior ribs are immediately apparent and oriented horizontally, each attaching to a thoracic vertebral body
- Anterior ribs are harder to see and are oriented downward toward the feet, attaching to the sternum
- Poor inspiration: compresses and crowds lung markings, especially at the bases leading you to think a lower lobe pneumonia exists → confirm with lateral XR
- Significant Rotation - may alter contour of heart, vasculature, hila, and hemidiaphragms based on the position of the patient
- Medial ends of clavicles are anterior and spinous process is posterior; should be equidistant from medial ends of clavicle on frontal XR
- If patient’s spinous process is closer to left clavicle → rotated toward R-side and vice-versa
- Marked rotation can make hilum appear larger → confirm with lateral XR or compare with previous XR
- Hemidiaphragm may appear higher on side rotated away from cassette → compare to previous study
- Remember: objects that are farther from the cassette are magnified compared to closer objects, always compare discrepancies to older XR or order a lateral
- Magnification - to assess the size of the heart
- The closer the object to imaging surface, the truer its actual size; farther it is, the more magnified
- Most CXRs are posteroanterior (PA) views - heart is closer (anterior) and truer to actual size
- This means the x-ray beam enters at P (posterior) and exits at A (anterior)
- Take Away: In AP image, heart is farther away and slightly magnified
- Angulation
- X-ray beam normally passes horizontally (parallel to floor) in upright XR, but hospitalized patients may not be able to sit up in bed
- Excessive angulation: clavicles will project at or above the posterior first ribs distorting the normal ‘S’ shape of the clavicle (makes them straight)
- May also make heart enlarged, mimicking cardiomegaly
- Sharp border of left hemidiaphragm may be lost, mimicking a pleural effusion or left lower lobe pneumonia → recognize artifacts and understand distortion, consult radiology
Normal Findings | Abnormal Findings | |
Penetration | Spine visible through the heart | 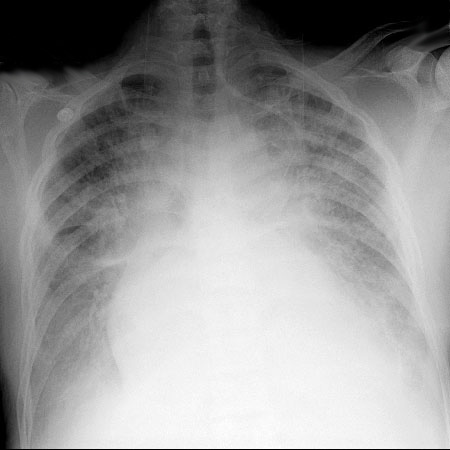 Ex. Underpenetration |
Inspiration | At least 8-9 posterior ribs visible | 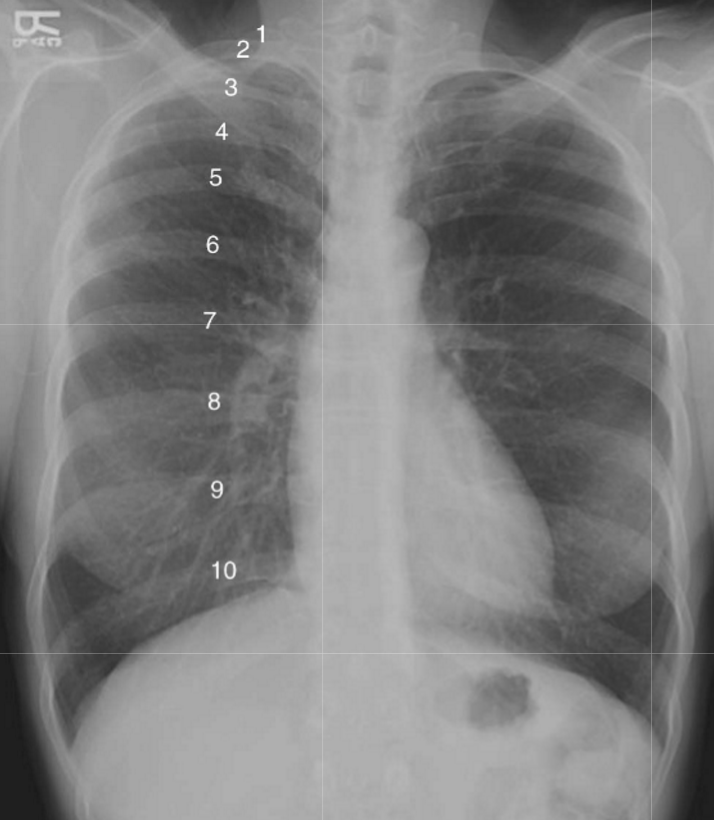 |
Rotation | Spinous process should be equidistant between medial ends of clavicles |  Hemidiaphragm appears higher on side rotated away (L) from cassette |
Magnification | AP films (most) will magnify heart |  |
Angulation | Clavicle has ‘S’ shape and superimposes on rib 3 or 4 | 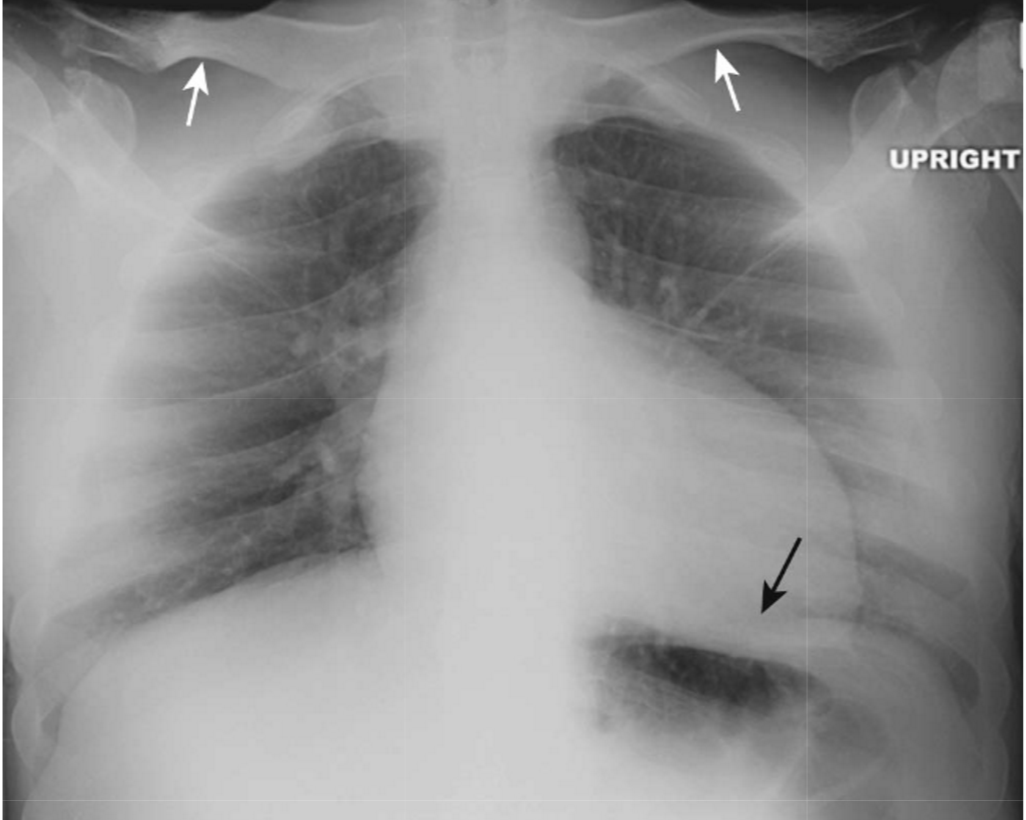 |
Sources
0 Response to "Introduction to Radiology for Physician Assistants"
Post a Comment